March 25, 2026
The goal of this article was to present a methodology to design and analyze an adaptive clinical trial with sample size recalculation at interim analysis, when the restricted mean survival time (RMST) is the primary endpoint. Especially, we focus on the situation of non-proportional hazards with a delayed treatment effect. Our aim is to provide trialists with new options to consider, to make better design choices, or to take better-informed decisions about design choices.
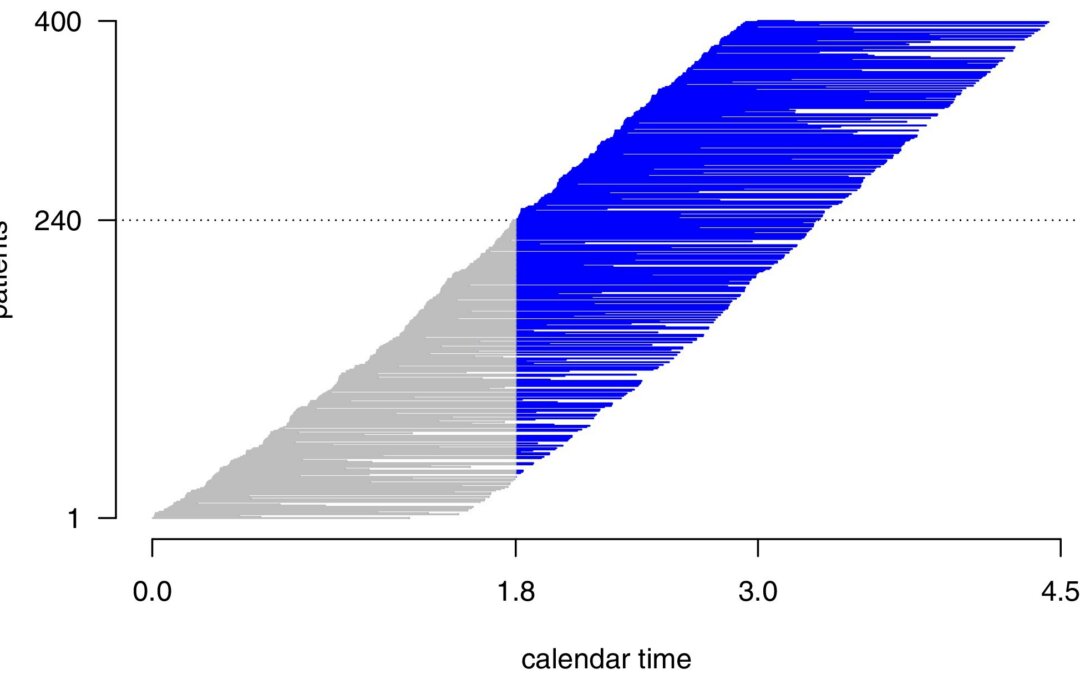
They consider an adaptive “two-stage” feature design of the trial. The first part consists of further follow-up data from patients who entered the trial before the interim analysis, but for whom further follow-up data were collected after the interim analysis. The second part comes from patients who entered the trial after the interim analysis. To define p-value critical values, they suggested to use the O’Brien-Fleming alpha-spending function approach. Sample size adaptations are made at the interim analysis. They also had to define a relevant tau, calculate relevant first stage sample size n1, and pre-specify reasonable weights, w1, and w2.
They ran simulation to compare their method to the log-rank test and a test comparing survival probabilities at tau years, studying the impact of timing of the interim analysis, and illustrating that the design can partly correct for wrong guesses during the initial planning. If the interim data suggested stopping early for efficacy or futility, the trial was stopped early but it if suggested continuing to the second stage, the sample size of the newly recruited patients for the second stage was determined using the conditional power principle. As long the conditional power at the second stage was greater than 80%, no further patients were recruited in the second stage and the test decision was based on the data from the interim analysis combined with the second-stage data, the latter consisting only of pipeline data. Else, the second-stage sample size was calculated as the smallest sample size such that a conditional power of at least 90% could be reached.
According to the authors, in terms of the performance of the simulations, first, type-I error rate compliance was assured under consideration of the Monte Carlo simulation error for all variants considered. Second, they found that their sample size recalculation could indeed mitigate the impact of incorrect initial guesses at the time of trial planning, in terms of suboptimal sample size and power. Their sample sizes were often reduced when initially assumed too large and often increased when initially assumed too small. They concluded from this that the worse the initial guesses, the larger the benefits of sample size recalculation turned out to be. Third, they said that the RMST-based approach attained smaller power values than the log-rank and -year survival approaches, as previously noted in the literature for scenarios with delayed treatment effects. Finally, fourth, the timing of the interim analysis did not substantially affect the power, but only the probability of early termination and the sample size of the second-stage data. They elaborated that one could expect that the more data available at the interim analysis and the more reliable the conditional power calculation, leads to observed power values closer to the target power. However, this was not observed in their simulation scenarios.
They did note that the three RMST-based approaches came along with a slight underpowering and also that in several scenarios, a power of 80% could not be reached by construction However, they said they saw that in the case of a too small initially planned sample size (cf. S9), an increase in overall power is possible with the new approach. Power values for their RMST-based approach were smaller than for the test comparing -year survival probabilities and the log-rank test, applied to the same sample sizes. Also, for these tests, the type-I error rates were maintained within the Monte Carlo error margins. They also demonstrated these items in a real dataset analysis.
Overall, they showed how to plan and analyze an adaptive trial with the RMST as the primary endpoint and they also provided the computational details for performing sample size recalculation at interim analysis, in the context of delayed treatment effect. They did this to provide new tools to plan trials in situations when non-proportional hazards are expected, and a large uncertainty about key parameters for sample size calculation is prevalent.
Written by,
Usha Govindarajulu
Keywords: survival, RMST, sequential, adaptive clinical trial, sample size calculation
References:
Hermann C and Blanche P (2026) “Sample Size Recalculation in Adaptive Group Sequential Study Designs for Comparing Restricted Mean Survival Times” Statistics in Medicine. https://doi.org/10.1002/sim.70490
https://onlinelibrary.wiley.com/cms/asset/b00b1046-d80f-44db-85fc-6c547772f00a/sim70490-fig-0001-m.jpg